What the Latest Data Shows
Because Down Syndrome carries multiple anatomical and physiological risk factors (for example, low muscle tone, narrow airway, large tongue, enlarged tonsils/adenoids, etc.), infants and toddlers are especially vulnerable. (MDPI)
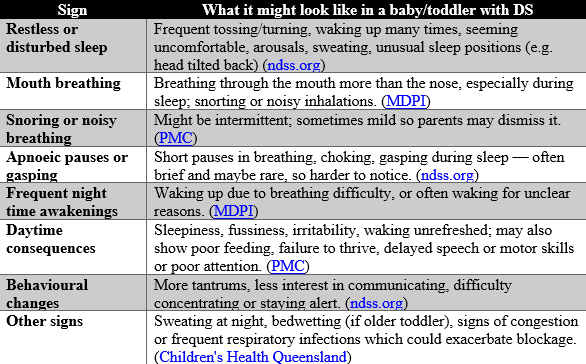
Subtle Signs of OSA in Infants & Toddlers with Down Syndrome
Many classic symptoms (e.g. loud snoring) may or may not be obvious; often the signs are subtle, especially in very young children.
Here are some signs to watch for:
- A recent 2024 study on a group of infants/toddlers with Down Syndrome, found that over 90% of the group had Obstructive Sleep Apnoea (OSA) even in their first year of life. (PMC)
- In preschool age (2-4 years), nearly all children with DS referred for sleep studies had OSA; only about 5% did not have the condition. (Paediatrics)
- The severity of OSA in these young children is also often high, with many showing moderate to severe obstruction and, in some cases, accompanying nocturnal hypoventilation or airway compromise. (Paediatrics)
Because Down Syndrome carries multiple anatomical and physiological risk factors (for example, low muscle tone, narrow airway, large tongue, enlarged tonsils/adenoids, etc.), infants and toddlers are especially vulnerable. (MDPI)
Subtle Signs of OSA in Infants & Toddlers with Down Syndrome
Many classic symptoms (e.g. loud snoring) may or may not be obvious; often the signs are subtle, especially in very young children.
Here are some signs to watch for:
For Parents and Parents-to-Be of Children with Down Syndrome
References
Disclaimer: The information provided on Small Steps Online is for educational purposes only and is not a substitute for professional medical, therapeutic, or developmental advice. Always consult with qualified healthcare providers, therapists, or relevant professionals regarding your child’s specific needs and situation. The September Institute and Small Steps Online are not liable for any outcomes resulting from the use or misuse of the information shared here.

Created with